An ECG Analysis Algorithm Designed Specifically for the Pediatric Population
Children differ from adults as to the types and characteristics of shockable and non-shockable ECG rhythms. The lower incidence of ventricular fibrillation (VF) in children indicates that they are more likely to have non-shockable rhythms than are adults. It is important to correctly classify non-shockable high-rate pediatric rhythms such as sinus tachycardia (ST), supraventricular tachycardia (SVT), and accelerated ventricular rhythms when presented to an AED used on a child. Adult-based AED arrhythmia analysis algorithms may have difficulty correctly classifying these high-rate pediatric rhythms as non-shockable since the characteristics of the non-shockable pediatric rhythms overlap the shockable criteria used in the adult-based algorithms.
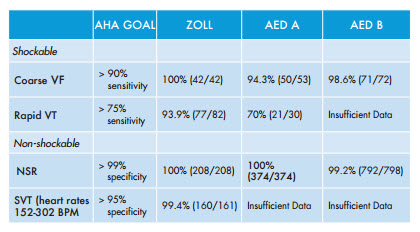
ZOLL has developed a dedicated pediatric AED arrhythmia analysis algorithm that accurately distinguishes shockable versus non-shockable pediatric rhythms even the most difficult high-rate, non-shockable rhythms. The analysis algorithm detects the use of either pediatric or adult therapy electrodes and automatically adjusts the arrhythmia analysis processing for the appropriate patient type. This algorithm is available in all ZOLL public access AEDs as well as in the ZOLL R Series. In the presence of pediatric electrodes, the unit automatically switches to pediatric mode, performs a complex rhythm analysis, and requires a heart rate for tachycardia of at least 200 beats per minute (BPM) to be considered shockable. Since SVT is a prominent pediatric arrhythmia, special efforts were made to gather a significant number of SVT rhythms during development of the ZOLL pediatric ECG algorithm. Adult-based algorithms typically consider high-rate SVT as a shockable rhythm; however, small children can have perfusing rhythms at these same rates but should not be shocked. The non-shockable rhythms in the database used by ZOLL included abnormal ventricular and supraventricular rhythms with rates up to 300 BPM, which are often found in infants and young children. Performance of the ZOLL pediatric arrhythmia algorithm on this database exceeded the performance recommendations the AHA has published for pediatric AED arrhythmia processing algorithms.12 The use of separate processing algorithms provides the means to retain a high-rate SVT in adults as a shockable rhythm while providing for pediatric SVT to be classified as non-shockable.
Although it is subject to the specifics of a given database, the ZOLL analysis algorithm demonstrated superior performance when compared to the performance reported in other pediatric AED studies that were based on the evaluation of adult-based algorithms on pediatric ECG signals.
Contrary to previous pediatric AED studies, shockable and non-shockable VT rhythms were more prominent than VF in our data collection. The database contained 122 records of shockable and non-shockable VT, as compared to 42 records of VF. The ability of the dedicated pediatric algorithm to detect these rhythms and recommend the appropriate therapy is a significant improvement over adultbased algorithms. The increased sensitivity in the detection of shockable ventricular tachyarrhythmia will reduce the time to cardioversion and the return to spontaneous circulation. The increased specificity in the detection of nonshockable VT rhythms will avoid unnecessarily shocking a pediatric patient who does not need defibrillation therapy.